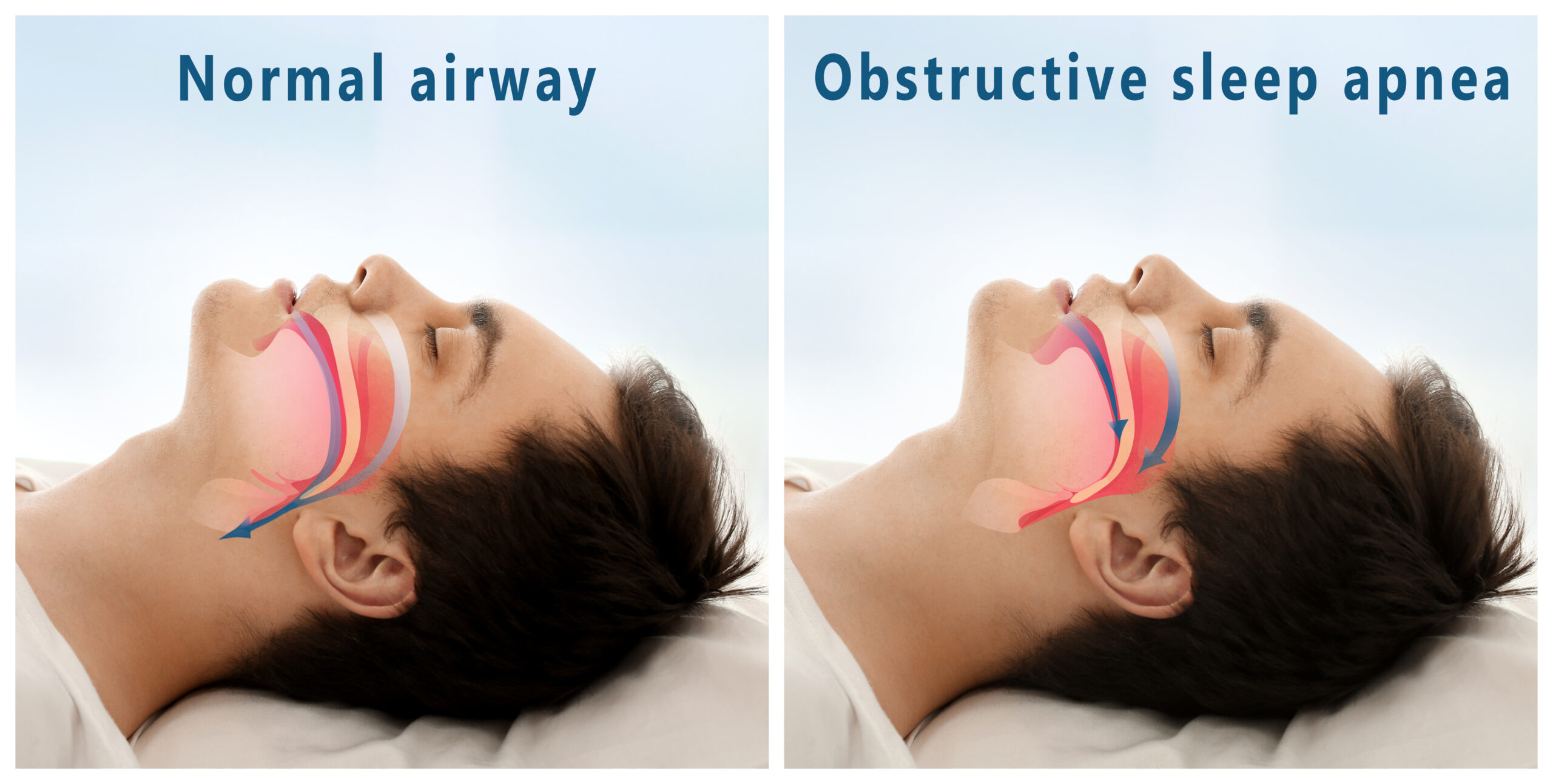
Anyone who has benefited from a sleep apnea oral appliance knows our bodies each have their own quirks, especially when sleep is involved. Obstructive Sleep Apnea, or OSA, links back to the shape and setup of your jaw, mouth, and throat.
Oral Appliance Therapy doesn’t work the same way for everyone. Why? Your jaws, teeth, and tongue all come together in a way that’s different for each person.
A sleep apnea doctor or specialist who handles sleep-related issues knows these tiny differences matter. They look closely at things like your jaw joint, the soft part at the back of your mouth, the shape of your throat, and even a small bone lower in your neck.
These pieces work together during sleep. If something is slightly out of place, it can close off your airway.
Oral appliances get custom-built to fit your mouth’s exact map. A slight tweak in jaw position can keep your throat open while you rest. Your dentist makes sure the fit isn’t just comfortable, but effective.
One person’s perfect fit might not work for someone else. Treating OSA is also about knowing your body’s blueprint.
A specialist trained for this job will spot details others might miss. This attention helps stop those nighttime breathing pauses so you get real rest.
Each small bone, soft tissue, and curve in your mouth shapes how well the therapy works. That’s why a personalized approach matters.
“There is now widespread recognition within the world of sleep medicine of the increasing importance of dental sleep medicine and, in particular, the role of oral appliance therapy (OAT) in the management of adults with obstructive sleep apnea (OSA),” states European Respiratory Society. “Whilst nasally applied continuous positive airway pressure remains the ‘gold standard’ in nonsurgical OSA management, OAT remains the recognized alternative treatment.”
The Interconnected Airway and Your Sleep Apnea Oral Appliance
Your jaw, teeth, tongue, and airway all work together in a unique way that supports a uniquely fitted sleep apnea oral appliance. No single part decides if oral appliance therapy (OAT) will work. Everything matters. Let’s say someone has a small lower jaw.
That can mean sleep issues. If their tongue is small and their jaw moves forward easily, OAT might help a lot. Another person with the same jaw shape but a large tongue or stiff joints could have trouble.
They may need special changes to their device. This is why doctors need to look at the whole mouth and throat before starting OAT.
Soft tissue acts differently at night. When you’re awake, muscles hold things in place. When you sleep, muscles relax.
The tongue and soft palate can fall back. This can block your airway. Tests done while you’re sitting up might miss this.
Drug-Induced Sleep Endoscopy (DISE) now gets used more often. DISE lets doctors watch what happens during sleep. They can see which parts collapse.
Only looking at the size of your airway isn’t enough. How it moves and shuts during sleep matters too. OAT’s success really depends on your unique setup inside your mouth and throat.
The Mandible and Tongue are Primary Targets for OAT
How well your sleep apnea oral appliance works depends on the shape of your head, jaw, and tongue. The lower jaw plays a huge role since most devices aim to shift it forward. Its movement range affects how well the therapy opens your airway.
Doctors check features like the angle of your jawbone. A flatter angle often means better results because moving the jaw forward can open the throat more. A steep angle might not help as much.
A set-back lower jaw, called retrognathia, can push the tongue back and block airflow. Mild to moderate cases often see real benefits from these oral devices. Moving the jaw and tongue forward gives your airway more space and can bring real relief.
You usually need at least 5 millimeters of jaw movement for best results. The device keeps your lower jaw forward during sleep, giving your tongue and throat more room.
The tongue matters a lot too. Its tendency to fall back at night is a common reason people struggle to breathe. Oddly, a bigger tongue doesn’t always spell trouble. For some, a large tongue actually means the device helps more, especially when the back of the tongue blocks the airway.
Doctors can use a jaw thrust test to see if this space improves, which hints at good chances with therapy. While one type of device pulls the jaw forward, another holds just the tongue. If your tongue is large because of extra fat, losing weight can help you breathe even easier at night.
Sleep Apnea Oral Appliance, Soft Palate, and the Hyoid Bone
Your soft palate and hyoid bone matter a lot when it comes to having success with any sleep apnea oral appliance. The back of the mouth, where the soft palate and uvula sit, is a trouble spot for snoring.
People with shorter soft palates tend to do better with MAD. If your soft palate is long, thick, or floppy, OAT may not work well for you.
Jaw thrust during DISE that opens the space behind the soft palate usually means OAT will help. DISE sometimes reveals a total collapse at the palate, which often predicts poor results. OAT affects the palate by moving the jaw and tongue, tightening the area, and making it less likely to collapse.
The hyoid bone looks like a horseshoe. It “floats” in your neck, held by muscles but not touching any other bone.
If the space from your lower jaw to the hyoid is small, OAT tends to work well. Wearing a MAD that brings the hyoid closer to the jaw often leads to fewer apnea events.
“The mandibular plane angle and the distance between hyoid bone and mandibular plane was found to have a predictive value for MAD effectiveness in OSA patients,” according to one study in the Journal of Clinical Sleep Medicine. “However, the relative weak and somewhat inconsistent cephalometric data suggest that decisions based solely on these factors cannot be recommended, especially because an integrated analysis of other risk factors (e.g., age, sex, BMI) should also be taken into account.”
OSA patients usually have a hyoid that sits lower and farther back, which narrows the airway. The hyoid bone anchors many muscles of your tongue and throat.
OAT works by shifting the jaw forward and, as a result, the hyoid too. This makes the lower airway more stable and open.
Lateral Pharyngeal Walls: A Sideways View of Airway Opening
Patients with sleep apnea oral appliance experience often talk about their tongue blocking the airway. However, few mention the sides of the throat.
These walls can actually block breathing for many with OSA. Knowing this helps predict if Oral Appliance Therapy will work.
Scan results show oral devices, especially MADs, make the throat wider, not just front to back. The biggest change happens sideways behind the soft palate. Tension from soft tissues connecting the throat’s side walls to the lower jaw seems to cause this.
The pterygomandibular raphe, a band connecting jaw to throat muscles, plays a role. Moving the jaw forward pulls these tissues outwards. This pulls the side walls open and helps breathing.
This mechanism matters most for people who don’t have tongue-driven airway collapse. Drug-Induced Sleep Endoscopy helps spot these collapse patterns. During DISE, moving the jaw forward can show if the side walls open more.
If the walls stay closed or only open a little, OAT probably won’t help. If a jaw thrust widens the airway, OAT might be a good choice.
In some cases, the side walls collapse together in a circle. This means the device might not help because the tissue is too weak or the forces squeezing the airway are too strong.
OAT’s effect on the side walls matters more than most people realize. It’s a key reason why these devices work for some, but not for everyone.
“Drug induced sleep endoscopy (DISE) has been established as a useful tool that can help determine patient candidacy for many of these interventions by way of assessing the anatomy and collapsibility of upper airway structures,” states the University of Iowa’s Carver College of Medicine. “DISE involves visualization of the upper airway with an endoscope during sedation mimicking a sleep state.”
TMJ Health During Sleep Apnea Oral Appliance Therapy
Your teeth and jaw joints play a big part in how well your sleep apnea oral appliance works and how comfortable it feels. Most oral devices need you to have enough strong teeth in both your top and bottom jaws, usually at least 6 – 10 inches each, spread out well. Back teeth help keep the device steady.
If you have gum disease, untreated cavities or very few teeth, regular oral appliances might not work for you. There is still hope if you have implants though, since those can sometimes hold the appliance in place.
Lots of dental work like crowns or bridges can make things tricky too. Your dentist needs to check carefully so nothing gets knocked loose.
Jaw joints matter a lot. They need to be in good shape to handle having your jaw pushed forward during OAT. Pain, clicking, or tightness in your joints should be checked before starting.
Some folks see their jaw issues improve with OAT. Others feel worse or get new problems. If you have a sore jaw now, OAT might not be an option.
OAT can bring some side effects. Most are mild. Morning jaw soreness, aching chewing muscles, popping in the jaw, sensitive teeth, more or less saliva, or irritated gums pop up sometimes.
Some people see changes in how their teeth fit together, especially the back teeth. That’s called a posterior open bite.
To fight this, patients often get a little plastic bite guide called an “AM repositioner” or do simple jaw stretches after removing the appliance. Your teeth and jaw joints don’t just need to start out healthy — they stay involved the whole time you use OAT.
Regular checks with your dentist help spot any changes early.
Feature and Type Comparison: A Helpful Breakdown
Here’s a Mandibular Advancement Device and Tongue-Stabilizing Device breakout table for comparison:
| Feature / Type | Mandibular Advancement Devices (MADs) | Tongue-Stabilizing Devices (TSDs) |
| Mechanism of Action | Gently push the lower jaw (mandible) and associated soft tissues (tongue, soft palate) forward, increasing airway space. | Hold the tongue in a forward position using suction, preventing it from collapsing into the throat. |
| Appearance | Resembles a custom-fitted sports mouthguard, typically covering both upper and lower teeth. | Often a bulb-like device with an opening for the tongue, positioned outside the teeth. |
| How it’s Held | Stays in place by fitting over the upper and lower dental arches. | Stays in place by suctioning onto the tip of the tongue. |
| Primary Use Case | Most common type for mild to moderate OSA. Also used for snoring. | Less common; often considered when MADs are not tolerated (e.g., edentulous patients, severe gag reflex with MADs) or for specific tongue-based obstructions. |
| Adjustability | Many custom-fitted MADs are adjustable, allowing for titration (incremental advancement) to optimize effectiveness. | Generally not adjustable in terms of tongue position, but fit can vary. |
| Patient Comfort | Generally good comfort, but can cause jaw discomfort, teeth soreness, or bite changes initially. | Can cause tongue soreness, numbness, or excess salivation. May feel less intrusive in the mouth overall than a full MAD. |
| Impact on Jaw/Bite | Can potentially lead to temporary or subtle permanent changes in dental occlusion (bite) over long-term use. | Minimal to no direct impact on jaw position or dental occlusion. |
| Speech with Device | Can be difficult or impossible to speak clearly with the device in place. | Speech is usually very difficult or impossible with the device in place. |
| Material | Typically made of acrylic, thermoplastic, or a combination of materials. | Often made of medical-grade silicone. |
| Maintenance | Requires daily cleaning, regular professional checks for fit and adjustment. | Requires daily cleaning. |
Broader Anatomical Influences on Airway Architecture
Other facial features can shape your airway and influence sleep apnea oral appliance therapy. Swollen tonsils or adenoids often block airflow, especially in kids.
Removing them sometimes stops OSA in children, though adults see less direct benefit. If big tonsils continue to block the airway after jaw movement, an oral device might not solve the problem.
Nasal issues like a bent septum or allergies force mouth breathing. This can push your tongue and palate back, making the airway even tighter. Good airflow through your nose helps these devices work better.
The shape of your skull base can play a part too. Research links a shorter skull base to less improvement with these treatments. A certain skull angle might make oral devices more effective.
Face shape matters more than most think. A shorter upper face or longer lower face often means better results from advancing the jaw. Your upper jaw’s width also counts.
A broad upper jaw tends to go with greater device success. But a narrow or high-arched palate limits tongue space and can make the nasal floor tighter, adding risk for OSA.
Some people who respond best actually start with narrow airway spaces — the areas that these devices open. If advancing the jaw and tongue clears the main blocked spot, you might see big gains.
Despite studies, it’s not always one feature that matters. Your combined facial structure tells the bigger story than any single measurement.
Biomechanics of Breathing and Your Sleep Apnea Oral Appliance
Your sleep apnea oral appliance will work by changing how your jaw and face are positioned. The appliance gently pulls your lower jaw forward.
This movement brings your tongue with it. The airway gets wider, not just front to back but side to side too. Imagine stretching out a bendy straw. It won’t squish as easily.
This added space makes it harder for your airway to close while you sleep. Muscles in your mouth see some changes too, but the main perk comes from opening things up. The pressure that shuts your airway drops, so breathing gets easier.
How far the jaw moves matters a lot. Move it a little and you might not see any change. Push too far and you risk jaw pain or tooth issues. Finding the right amount for you is key.
A one-size-fits-all device just won’t work. The appliance needs to be adjustable. Each person’s facial bones and comfort levels are different.
Some people have other issues that make their sleep trouble worse. Their throat might collapse easily, or they might wake up at the smallest noise. The jaw appliance might help, but sometimes it’s not enough on its own. Mixing in other treatments can help get better sleep.
The bottom line? If your airway can handle the jaw shifting and your body responds well, you’ll get good results with Oral Appliance Therapy.
If your sleep problems are more complicated, you might need a few tools working together. Getting a device made just for your mouth makes all the difference.
Wellness and Pain
Personalize your sleep apnea oral appliance by visiting Wellness and Pain. We offer conservative treatments, routine visits, and minimally invasive quick-recovery procedures. We can keep you free of problems by providing lifestyle education and home care advice.
This enables you to avoid and manage issues, quickly relieving your inhibiting lifestyle conditions when complications arise. We personalize patient care plans based on each patient’s condition and unique circumstances. Wellness and Pain can help improve wellness, increase mobility, relieve pain, and enhance your mental space and overall health.